Introduction – Searching for Context
In the previous post, I talked about my personal experiences of an eating disorder, which began as binge eating disorder, then developed into mild anorexia. In this article, I’m going to be exploring the context of its development in relation to the rise of eating disorders in the 20th century and their prevalence at this time. I will begin by outlining what eating disorders are and how the different types of eating disorders are currently defined. I will then provide a brief history of eating disorders, focusing on how the shift of cultural ideals from fuller forms towards thinness has led to their proliferation over the last century. I shall discuss how the flawed BMI model has led to the demonisation of obesity and to healthy people being shamed as overweight and obese and to developing eating disorders. I will then talk about the disturbing phenomenon of the deification of anorexia as the goddess Ana, within the pro-Ana movement. Finally, I will focus on how the decline of religion in Western Europe has led to size becoming a religion, with its own commandments on food and exercise, as voiced by new idols on social media.
What is an Eating Disorder?
An eating disorder is defined by the Oxford Language Dictionary as ‘any of a range of mental conditions in which there is a persistent disturbance of eating behaviour and impairment of physical or mental health.’
Eating disorders often develop as ways of managing difficult or overwhelming emotions that stem from stress and trauma. They can be precipitated by dieting and may or may not be related to cultural ideals of thinness.
An eating disorder differs from dieting and other forms of disordered eating such as skipping meals, in terms of the severity, frequency and duration of the symptoms, the levels of psychological and physical stress, and the impact on the person’s capacity to function and their relationships.
The Types of Eating Disorder
The main types of eating disorder are anorexia, bulimia, and binge eating disorder. In the UK, two resources are used to diagnose eating disorders: the Diagnostic and Statistical Manual of Eating Disorders, 5th Edition (DSM-5) and the International Classification of Diseases, 11th Edition (ICD-11).
Anorexia is defined by ‘the restriction of energy intake relative to requirements leading to a significantly low body weight’, ‘intense fear of gaining weight’ and disturbance in perception of body weight and shape. Other symptoms include: amenorrhea, digestive issues, dizziness, fainting, feeling cold and numb, poor circulation and dry skin. In severe cases, anorexia can lead to osteoporosis, organ failure, cardiac arrest and death. Around 5% of patients with anorexia die within four years of receiving a diagnosis.
The main diagnostic criteria of bulimia are ‘episodes of binge eating’ followed by ‘inappropriate compensatory behaviour’. Binge eating is defined as eating within a 2-hour period ‘an amount of food that is definitely larger than what most individuals would eat in a similar period of time under similar circumstances’ and by ‘a sense of lack of control of overeating during the episode’. Compensatory behaviours include: vomiting, misuse of laxatives, fasting and excessive exercise. These episodes are driven by concerns about body weight and shape. They must take place at least once a week for three months to warrant a diagnosis. Other symptoms are similar to anorexia and self-induced vomiting can also cause a sore throat, swollen glands, tooth erosion, Russel’s sign on the hands and electrolyte imbalances.
The diagnosis of binge eating disorder is also based upon ‘recurrent episodes of binge eating’. These are not followed by compensatory behaviours. Binge eating episodes must be associated with three or more of the following criteria: ‘eating much more rapidly then normal, eating until feeling uncomfortably full, eating large amounts of food when not feeling physically hungry, eating alone because of feeling embarrassed by how much one is eating, feeling disgusted with oneself or very guilty afterward’. Marked distress about the binge eating must be present and the episodes must take place at least once a week for at least once a month. Binge eating disorder can lead to excessive weight gain and thus to high blood pressure, high cholesterol levels, breathing issues, joint problems, digestive diseases such as gallstones and gallbladder disease and type two diabetes.
There are also a number of Other Specified Eating and Feeding Disorders (OSFED). These include atypical anorexia wherein ‘the criteria for anorexia are met, except that despite significant weight loss, the individual’s weight is within or above the normal range’, bulimia (of low frequency and/or limited duration), binge eating disorder (of low frequency and/or limited duration), purging disorder, night eating syndrome, pica, rumination disorder, Avoidant/Restrictive Food Intake Disorder (AFRID), orthorexia and Unspecified Feeding or Eating Disorder (UFED).
A History of Eating Disorders
It’s likely that humans have restricted food intake, binged, purged, and over-exercised as a form of relief from stress and trauma since we have existed. However, for the most part, people did not engage in such behaviours to be thin.
Venus figurines, with large bellies, breast and hips, suggest that larger body shapes were idealised during prehistoric times. This might relate to food scarcity and to larger forms being associated with fertility and survival.


Religious fasting has long been a common practice and differs from an eating disorder as it involves a conscious choice to bring a person closer to the divine rather being a coping mechanism or a method of weight loss. However, it can develop into an eating disorder when it becomes an addiction and spirals out of control and manifests as self-starvation.
From the Hellenistic period, we have the first records of religious fasting being taken to the extremes of emaciation and starving. Blaesilla, a Roman woman who followed the ascetic practices of Saint Jerome, starved herself to death. This has been interpreted as an early example of anorexia.
We also find examples of binging and purging that bear similarities to bulimia in wealthy cities such as Ancient Rome. The Roman emperor, Vitellius, was renowned for having three or four feasts a day, made possible by his vomiting. The emperor, Claudius, never left a meal until overfed, after which ‘a feather was placed in his throat to stimulate his gag reflex.’ These behaviours have more to do with gluttony – emptying one’s belly in order to fill it with more food – than with bulimia as a mental illness outside their control.
In medieval times, extreme ascetic practices remained common. Around the 10th century, Saint Wilgefortis, ‘bearded virgin’, starved herself to avoid marriage, leading to hair growing all over her body (a phenomenon known as languo – the body’s response to fat loss in order keep warm), including her face, leading to her growing a beard. Saint Catherine of Siena famously starved herself to death in 1380, attempting to survive only on the eucharist. This phenomenon has been referred to as anorexia mirabilis ‘holy anorexia’.


Intriguingly, in medieval tales wild men and woman who become geilt or wyllt ‘mad’ such as Suibhne Geilt, Mis, Myrddin Wyllt, and the knight, Owain, who retreat in madness into the wilderness, are described as hairy. This, no doubt, was caused by them living in a state of near-starvation. Living in the wild and extreme fasting are associated with initiation in some cultures. This might be seen as a temporary state of anorexia, which reaches an end when the person has a religious experience and returns to their community.
The illness we now know as anorexia nervosa was first described by Richard Morton, in 1689, in relation to a male and female who lost their appetite and wasted away without physical explanation from nervous consumption. The term anorexia nervosa (a nervous loss of appetite)was coined by William Gull in 1873 in relation to case studies of young women, aged 16 – 23, who suffered from fatigue, loss of body mass and weakness.
These diagnoses bore no relation to societal ideals of thinness. Up until the nineteenth century, the ideal female body shape was curvy and voluptuous, as shown by statues and paintings of women with fuller figures. It was during the Victorian period that slimmer ideals came into vogue, with hourglass figures, and women cinching in their waists with corsets.
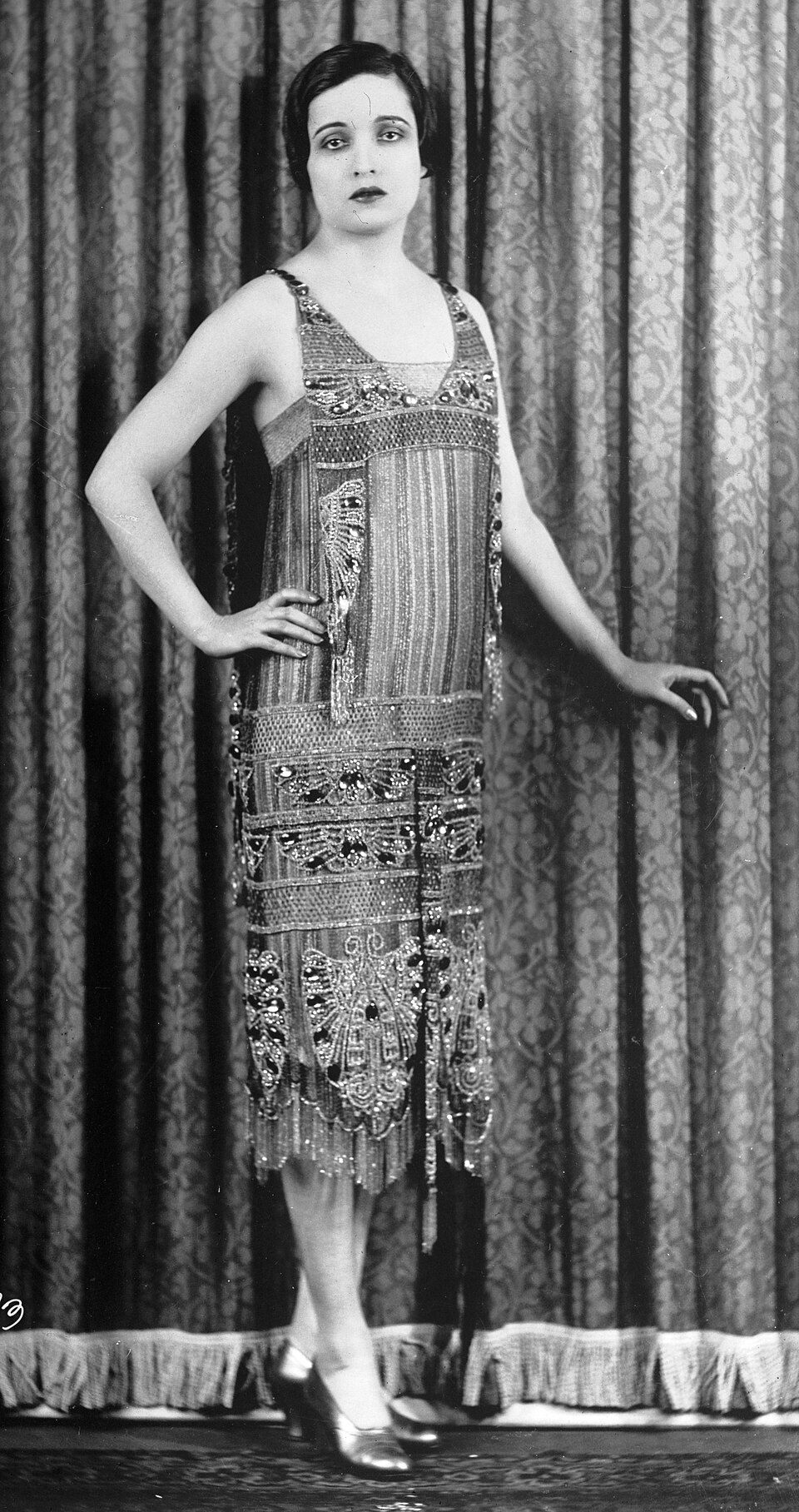
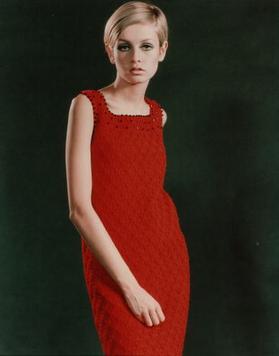
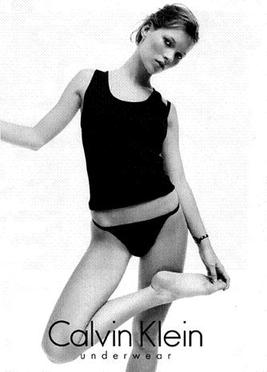
The thin ideal came into being in the 1920s with the flapper image focusing on a slender, boyish shape. In the 1960s, Twiggy provided the defining look. The apogee was the 1990s, when extreme levels of thinness were reached, with waif-like, clinically underweight models, referred to as heroin chic.
The first case studies of binging and vomiting were recorded by Bliss and Branch in the 1960s, and by Ziolko during the 1970s. In 1979, Gerald Russell coined the term bulimia nervosa (bulimia means ‘ox-hunger’ and the term has been translated as ‘ravenous appetite’)in a paper covering 30 cases. Binge eating disorder was first described in 1959 by the psychiatrist, Albert Stunkard.
During the 1970s, an ‘epidemic of obesity’ was declared. People were labelled as overweight or obese and this led to many developing eating disorders.
A sudden rise in eating disorders, driven by the derogation of fat bodies and the glamorisation of near-anorexic bodies, was seen between the 1960s and 1990s. Their prevalence has risen even more sharply, by 15%, since 2000. This has been driven by the anxiety and social isolation of the COVID pandemic and by the influence of social media promoting unhealthy ‘thin’ and ‘fit’ ideals. A 2017 study by Hay, in the UK, found that that 8% of the cases were diagnosed with anorexia, 19% with bulimia, 5% with binge eating disorder, 5% with ARFID, and 47% with OSFED.
The Demonisation of Obesity
Unfortunately, fat-shaming has been around for a long time. In Spartan Greece, between the 6th and 2nd centuries BCE, slim, muscular physiques were favoured and fat people were shamed and even fined.
However, this was not the norm across cultures and history. Generally, fuller forms that were able to survive food shortages and harsh weather were lauded. In Western Europe, it was only during the nineteenth century, when the food supply became better, that a thin-waisted female figure was promoted and fatness became seen as a moral failing, associated with laziness and lack of self control. This was bound up with colonial values. Larger Black and Brown bodies were seen as dirty and undisciplined.
As the food supply has increased, so have the divisions between the cultural ideal of the thin white person and its antithesis – the fat (often Black) person. This has reached its height with the discourse around an ‘epidemic of obesity’.
Since the 1970s, obesity has been framed as a major health issue, stemming from unhealthy eating habits and a lack of exercise and associated with poverty. ‘Morbidly obese’ people, frequently depicted in the media as being lifted from their homes by ‘bariatric rescues’, are often seen as objects of ridicule and portrayed as being of demonic proportions.
In a 2025, in a report from the House of Commons Library on ‘Obesity Statistics’, 31% of women and 39% of men were labelled as overweight and 30% of women and 28% of men as obese. Adult obesity prevalence was shown to have risen from 15% in 1993 to 29% in 2022. This was shown to be associated with social deprivation, disability, ethnicity (‘people in Black ethnic groups have the highest rates of excess weight’) and a lack of education.
This discourse is based on the faulty BMI model hat originated as ‘the Quetelet index’ in 1932 when the Belgian sociologist, Adolphe Quetelet, designed the weight-to-height ratio (kg/m2) to define the ‘average man’ and measure population norms. Notably, it was created by a white man to find a norm amongst other white men. The term Body Mass Index (BMI) was coined in 1972 by Ancel Keys and used it as a tool for population studies on obesity.
Quetelet never intended his model to be used to used to measure individual health or body fat. It has increasingly been criticised because it does not take into account muscle mass, bone density or different body types.
Self-identified fat doctor, Astrıður Stefa´nsdottir, who, according to the BMI scale is overweight, yet is perfectly healthy, points out how the current ‘scientific’ position has led to fat people who are in in control of their fates in ‘the kingdom of the well’ being reduced to ‘patients’ in ‘the kingdom of the sick’ ‘under the management of medical personnel’.
During the 1960s, the Fat Liberation movement arose. This was deeply intertwined with the Black Rights movement. Both critiqued the hegemony of thin, white ideals and called for equal rights for fat and Black bodies. This has more recently developed into the Body Positivity movement and has led to the establishment of groups such as Health at Every Size (HAES) whose core principles are: weight inclusivity, health enhancement, respectful care, eating for well-being, and life-enhancing movement.

The Deification of Anorexia
On the other extreme, the pro-anorexia or pro-ana movement began developing online in the early 2000s. Therein, anorexia is re-conceptualised as a lifestyle choice as opposed to an illness and is seen as a skill and as a religion.
These sites provide ‘thinspiration’ and actively encourage followers to under-eat and over-exercise, casting this in terms of self-discipline, and providing weight loss tips. ‘Anorexia is a skill, perfected by only a few. The chosen, the pure, the flawless.’ ‘Watch other people eat and feel superior. You don’t need that food!’ ‘The pain is necessary, especially the pain of hunger. It reassures you that you are strong, can withstand anything.’ They actively deny the danger to health and longevity of anorexia. ‘The bests anas never die.’
Anorexia is, even more disturbingly, portrayed as a religion with its own ruling goddess, Ana. She is viewed as a creator: ‘I (Ana) have created you, this thin, perfect, achieving child.’ She has her own version of the Ten Commandments, the Thin Commandments, such as ‘Thou shalt not eat without feeling guilty’. She is also viewed as a demoness who haunts and possesses.
This toxic online movement has led to people with anorexia seeing their illness as a lifestyle choice that lifts them above the herd, elevating them into a community who view themselves to be superior to the rest of food-eating society. This makes them less likely to seek treatment and can lead to death.


Size and Shape as Religion
Having studied the context, I now understand better the cultural milieu in which my eating disorder developed. I grew up in a Christian country with nominally Christian parents but, hating church parade with Brownies, reached the conclusion that the Christian God was not my God and didn’t entertain the thought that there might be others until I entered my mid-twenties.
My primary school was not religious. Instead, it was ruled by size and shape. A tubby child with a pot belly, I was bullied ruthlessly, called a ‘pig’. Comfort eating, due to bullying, led to binge eating, and I became overweight.
I’m not sure how long fat people have been identified with pigs. Wild boar and pigs are, contrarily, revered and cast as destructive in the Celtic tradition. Although swine were likely always seen as boisterous and as having voracious appetites, I imagine that it was not until they were penned that they were associated with dirtiness and laziness. How long insults such as ‘fat cow, ‘sow’ or ‘pig’, ‘eat like a pig’ and ‘pig out’ have existed, I remain uncertain.
During primary school and throughout high school, during the 1980s and 1990s, the female ideal did not seem to be based so much on skinny catwalk models as the Playboy or Barbie Girl aesthetic symbolised by Pamela Anderson. It was thin, blonde, tanned, with big boobs. Many of the girls at school bleached their hair, wore orange foundation and fake tan, lots of mascara and push-up bras. I didn’t adhere to this ideal. My first attempts to lose weight, at the age of thirteen, were driven more by the desire to evade bullying and to look like the thinner riding instructors at my riding school.
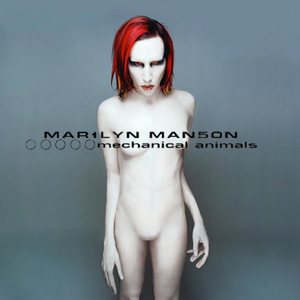
It was only when I started college that I started looking for ‘thinspiration’ to cultural idols. Again, these were not the thin female models from the catwalk. They were male figures from the eighties, rock and goth scene, such as David Bowie, Marilyn Manson and Richey Edwards, who sported an androgynous look. Looking back, this strikes me as odder than I remember, and leads me to the conclusion that I’m slightly gender fluid.


At this time, I lost about three stone in six months, then continued to eat a restrictive diet, but yo-yoed up and down for a number of years due to binge eating and binge drinking, until I managed to get the binge eating under control. As my eating disorder shifted entirely into mild anorexia, I became underweight.
Androgyny suited my body because I’m naturally a rectangle shape with small breasts, not much of a waist, narrow hips and longish legs. I found that, when I gained weight mainly due to binge drinking, fat gathered around my stomach and on my face, making me look like a round-faced barrel on legs. When I lost weight again, I emulated a thin runner’s ideal. At present, at my ideal weight, eating healthily and strength training, my figure is more athletic and remains boyish.



As a gym-goer I could say a lot about the religion of shape and size in gyms. In the 2010s, following the 2012 Olympics, the ‘strong not skinny’ movement formed a shift away from thinness towards strength and athleticism. This values function over form, body diversity, and mental strength. It celebrates a number of body shapes such as ‘toned’, ‘fit’ and ‘built’. Yet, ‘thick toned hour-glass figures’ for women, with narrow waists and well-developed glutes and thighs, have become the new ideal. This is something I certainly can’t achieve.
The ‘strong not skinny’ movement has been subject to critique due to its exclusion of thin people and replacing one unrealistic standard, thinness, with another, fitness, when the latter is difficult to attain for people with busy lives. It has also been seen as promoting restrictive dieting and excessive exercise.
Personally, I’ve found it’s helped me shift from being thin to being stronger and healthier. When I go to the gym, I don’t feel pressured to fit into any ideal. What I love about my gym is that there are bodies of all shapes, sizes and colours there, together, working out, without criticism or judgement.
A Better Religion
In Goodbye Ed, Hello Me, (ED stands for eating disorder), Jenni Schaefer writes about how she did not manage to recover from her eating disorder fully until she found God. ‘I now know that a complete, full life for me means not only saying good-bye to Ed but also saying hello to God. I don’t think I would ever have been able to fully love myself without letting God into my life. First I let others love me, then God, and finally I was able to love myself.’
Similarly, finding my religion, Brythonic polytheism, and developing a loving relationship with my patron God, Vindos / Gwyn ap Nudd, has helped me to recover from my eating disorder and from alcohol dependency.
As I have served Him through my writing and shamanic work, Gwyn has made it increasingly clear that I need my body to be a strong vessel for inspiration from Him and my spirits. I need to be in good to health for Them and my clients. This means neither binge eating or drinking, nor restricting, nor exercising excessively. The latter is the hardest because I’ve got a hyper-active nervous system and exercise is my most effective form of stress relief. I also really enjoy it and, if I’m having a good day, I can get carried away. If I do over-exercise, I try to do my best to eat something to make up for it.
Conclusion – A Body in Service
It’s said that one of the keys to recovering from an eating disorder is shifting from how one’s body looks to what one’s body can do. I’m certainly at my happiest and have the least eating disorder thoughts when I’m immersed in something I love, whether that’s working out at the gym, writing, praying, meditating, doing shamanic work or going for a walk in my local area. This is all good so long as it’s done from a desire to serve my Gods and not to get thin, burn calories, restrict my appetites, or take my stress out on my body.
A question I keep coming back to is: ‘Who am I serving? My Gods or the ED?’
Each time I notch up a score for my Gods, I feel closer to full recovery.
SOURCES
DSM-5-TR Diagnostic Criteria for Eating Disorders, https://insideoutinstitute.org.au/resource-library/dsm-5-diagnostic-criteria-for-eating-disorders
ICD-11, https://icd.who.int/en/
Beat Eating Disorders, https://www.beateatingdisorders.org.uk/
Health at Every Size, https://asdah.org/haes/
Obesity Statistics, House of Commons Library, 2025, https://commonslibrary.parliament.uk/research-briefings/sn03336/
Knapton, O., ‘Pro-Anorexia: Extensions of Ingrained Concepts,’ Discourse & Society, vol. 24, no. 4, (2013), JSTOR, http://www.jstor.org/stable/24441481
Mulheim, L., ‘History of Eating Disorders’, Very Well Mind, (2026), https://www.verywellmind.com/history-of-eating-disorders-4768486
Schaefer, J., Goodbye Ed, Hello Me: Recover from your Eating Disorder and Fall in Love with Life, McGraw Publications, (2009)
Stefa´nsdottir, A., ‘Three positions on the fat body: Evaluating the ethical shortcomings of the obesity discourse’, Clinical Ethics, Vol. 15, (2020), https://journals.sagepub.com/doi/10.1177/1477750920903455
Valentine, S., ‘Ancient Hunger, Modern World,’ Aleph, 19, (2022), https://www.researchgate.net/publication/363244110_Ancient_Hunger_Modern_World
